On This Page
- What Is a Whipple Procedure?
- Who Is Eligible?
- Who Is the Best Surgeon for a Whipple?
- Questions to Ask the Surgeon
- What Happens During the Procedure?
- What Happens After Surgery?
- Are Other Treatments Given with the Whipple Procedure?
- Long-Term Effects

What Is a Whipple Procedure?
The Whipple procedure, or pancreaticoduodenectomy, is the most common surgery to remove tumors in the pancreas. Surgery to remove a tumor offers the best chance for long-term control of all pancreatic cancer types. The Whipple removes and reconstructs a large part of the gastrointestinal tract and is a difficult and complex operation.
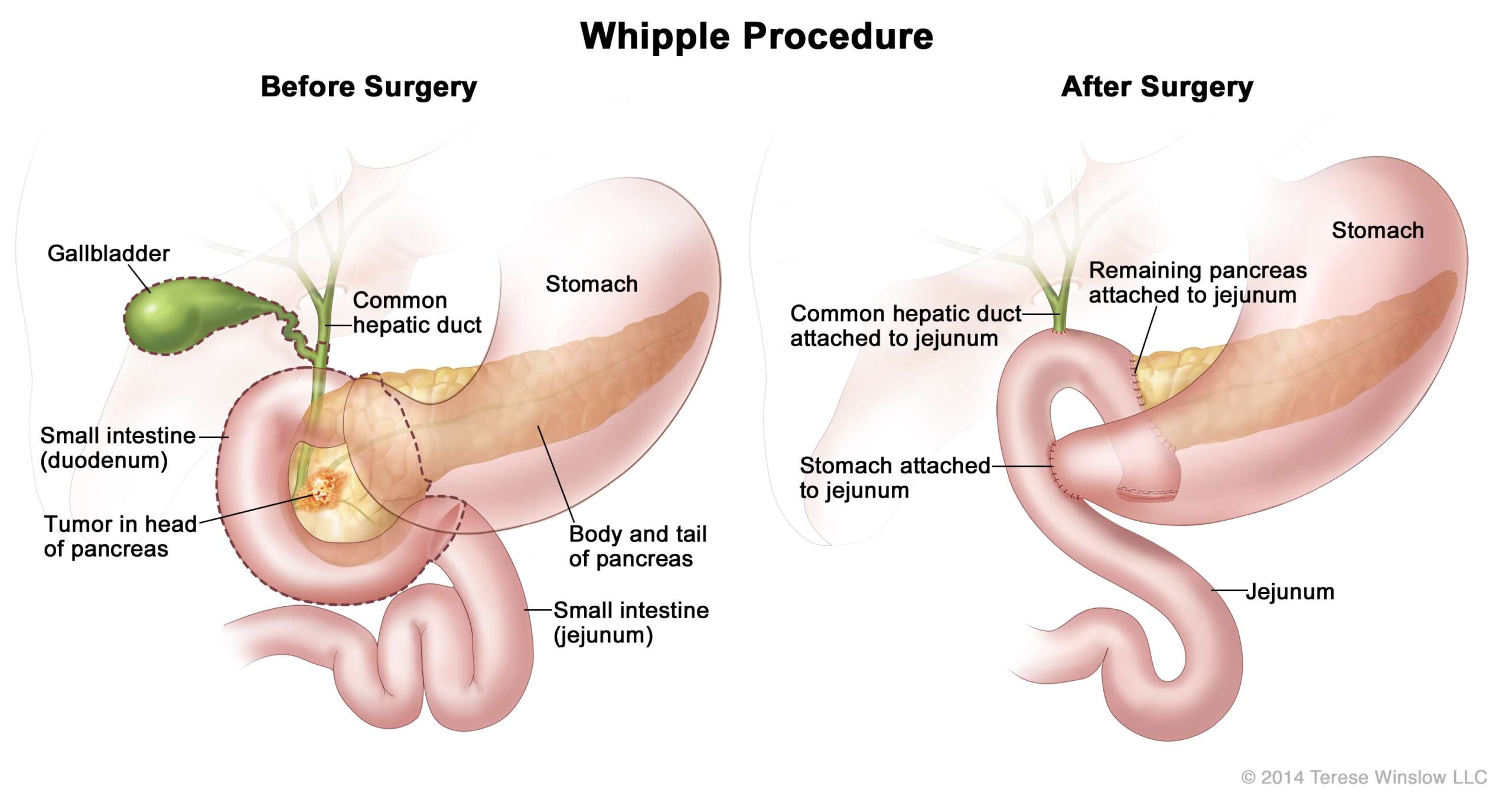
Before Surgery: This figure shows a tumor on the head of the pancreas prior to surgery. After Surgery: This figure shows the re-attachment of the common hepatic (bile) duct, remaining pancreas and stomach to the small intestine (jejunum).
Who Is Eligible?
The Whipple procedure may be attempted if the tumor:
- Is in the head of the pancreas.
- Has not spread to other parts of the body.
- Can be safely removed without causing damage to important blood vessels.
Although 20 percent of pancreatic cancer patients may be eligible for surgery, data shows that up to half of those patients are told they are ineligible. The Pancreatic Cancer Action Network strongly recommends you see a surgeon who performs a high volume of pancreatic surgeries (more than 15 per year) to determine eligibility.
Determining a patient’s eligibility for surgery is not always easy. Even sophisticated imaging tests may not provide perfect information. In some cases, despite testing before surgery, the surgeon may find during the procedure that the cancer has spread or cannot be removed. Therefore, the planned operation cannot be completed.
Who Is the Best Surgeon for a Whipple?
Pancreatic surgery is very complicated. Data show high volume surgeons at high volume hospitals have higher success rates and fewer complications. The Pancreatic Cancer Action Network strongly recommends you have a high volume pancreatic surgeon (more than 15 surgeries per year) perform the surgery.
PanCAN Patient Services can provide more information, including a list of institutions and doctors who perform a high volume of pancreatic surgeries.
Questions to Ask the Surgeon
- Can my tumor be removed through surgery? Why or why not?
- How many pancreatic surgeries have you performed? How many in the past year?
- How many pancreatic surgeries are performed at your hospital every year?
- What are the possible complications of pancreatic surgery?
- How long should I expect to be in the hospital recovering after pancreatic surgery?
- Would you be able to recommend another experienced surgeon for a second opinion?
- What will my life look like after surgery?
What Happens During the Procedure?
In a standard Whipple procedure, the surgeon removes the head of the pancreas, the gallbladder, the duodenum, a portion of the stomach and surrounding lymph nodes. The surgeon then reconnects the remaining pancreas and digestive organs.
In some cases, patients may undergo a modified version of the Whipple procedure, which keeps the entire stomach and the stomach valve called the pylorus. This is called a pylorus-preserving Whipple.
Both types of surgery typically take 5-7 hours.
What Happens After Surgery?
The patient stays in the hospital for 8-10 days after a Whipple procedure. During this time, doctors watch for complications, and the patient slowly begins drinking and eating again.
In the days following surgery, doctors run extensive tests to see if all the cancer was removed and if any cancer cells were in the lymph nodes.
After a Whipple procedure, the most common complication is delayed gastric emptying. This means the stomach takes too long to empty its contents. Usually, after 7-10 days, the stomach begins to empty well enough to allow healing. If delayed gastric emptying continues, the patient may require feedings through a feeding tube or vein for several weeks.
The most serious potential complication of a Whipple procedure is abdominal infection due to leakage where the pancreas is connected to the small intestine. This is referred to as a pancreatic leak or pancreatic fistula. This occurs in about 10 percent of patients and is usually controlled with a combination of draining tubes and antibiotics. Many of these patients require nutritional support.
Are Other Treatments Given with the Whipple Procedure?
Sometimes, patients receive treatment before surgery. This is called “neoadjuvant therapy,” and it is usually chemotherapy, radiation therapy, or both.
Often patients receive “adjuvant therapy”, or treatment that is given after surgery. The goal is to kill any small cancer cells that may still be present to prevent the tumor from coming back.
Clinical trials may be available for pancreatic cancer patients seeking neoadjuvant or adjuvant therapy.
Long-Term Effects
The Whipple procedure may cause challenges, including digestive difficulties, for a long time.
- It can take a patient anywhere from a few months to a year to feel relatively “normal” again.
- It takes time for the digestive system to start working again, and some patients must make permanent diet changes to reduce symptoms such as diarrhea, gas and stomach pain.
- Many patients also take pancreatic enzymes to help digest food properly.
PanCAN Patient Services can provide resources and information about challenges after surgery, including diet and nutrition information.
We’re Here to Help
For free, in-depth and personalized resources and information on pancreatic cancer, contact PanCAN Patient Services.
Related Topics
-
Pancreatic Cancer Specialists
Understand why it is important to see a pancreatic cancer specialist for your care.
-
Diet Changes After Whipple
See some general nutrition guidelines for post-Whipple patients.
-
Other Types of Treatment
Learn about other ways to treat pancreatic cancer.
Information reviewed by PanCAN’s Scientific and Medical Advisory Board, who are experts in the field from such institutions as University of Pennsylvania, Memorial Sloan-Kettering Cancer Center, Virginia Mason Medical Center and more.
Information provided by the Pancreatic Cancer Action Network, Inc. (“PanCAN”) is not a substitute for medical advice, diagnosis, treatment or other health care services. PanCAN may provide information to you about physicians, products, services, clinical trials or treatments related to pancreatic cancer, but PanCAN does not recommend nor endorse any particular health care resource. In addition, please note any personal information you provide to PanCAN’s staff during telephone and/or email communications may be stored and used to help PanCAN achieve its mission of assisting patients with, and finding cures and treatments for, pancreatic cancer. Stored constituent information may be used to inform PanCAN programs and activities. Information also may be provided in aggregate or limited formats to third parties to guide future pancreatic cancer research and education efforts. PanCAN will not provide personal directly identifying information (such as your name or contact information) to such third parties without your prior written consent unless required or permitted by law to do so. For more information on how we may use your information, you can find our privacy policy on our website at https://www.pancan.org/privacy/.

